颗粒细胞瘤
Granular Cell Tumor,GCT
同义词(或曾用名): 颗粒性肌母细胞瘤、颗粒细胞神经鞘瘤、颗粒细胞神经纤维瘤
概述:
由具有雪旺细胞分化,胞浆内含有嗜伊红色细颗粒状的圆形或多边形细胞组成的良性肿瘤。
发病部位: 头颈部最常见,特别是舌和口腔,其次乳腺及其他实质脏器也可发生。
诊断要点:
多发生于 40-60 岁成年人,男性略多见;头颈部最常见,特别是舌和口腔,其次乳腺及其他实质脏器也可发生;多表现位皮下的孤立性无痛性结节,偶见多灶发生;
肿瘤多见于皮肤和皮下组织,亦可见于黏膜部位和肌内或内脏器官,界限不清楚,无包膜,质软,实性,灰白、灰黄色;
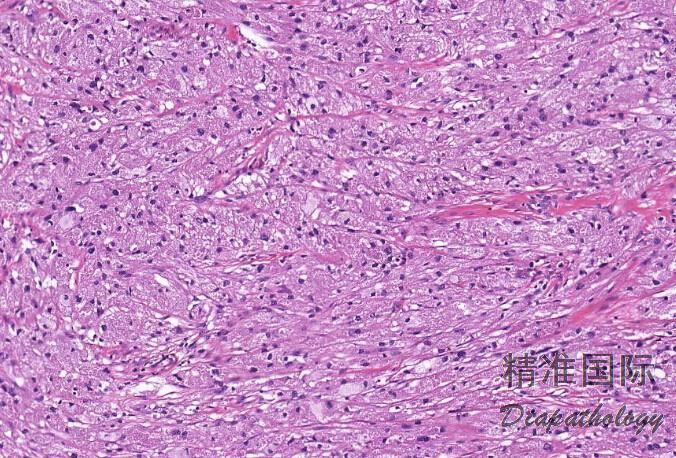
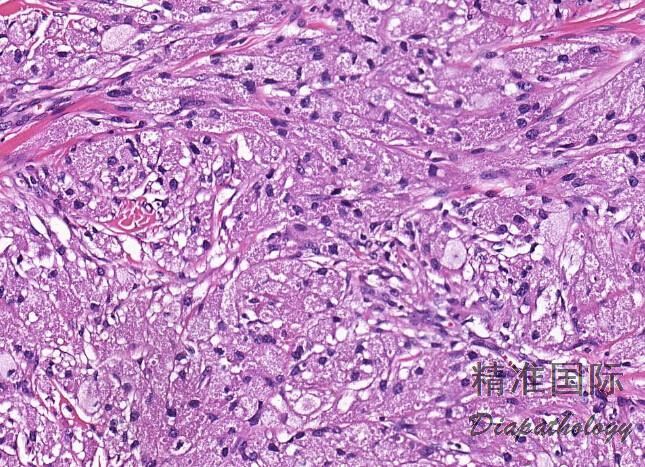
肿瘤细胞呈巢状、簇状或成片的上皮样细胞胞质呈嗜伊红色细颗粒状,部分可见到嗜酸性小球 PAS 染色阳性;
肿瘤细胞间为宽窄不等的纤维结缔组织间隔;瘤细胞成片状或条索状分布在胶原纤维束之间;
瘤细胞核通常小而深染,有时可见较大呈空泡状的核,通常罕见核分裂象,无坏死;
6.30%的病例可见表覆鳞状上皮呈现假上皮瘤样增生;
- Fanburg-Smith 等根据以下 6 个组织学特征对皮肤颗粒细胞的生物学行为进行分类,包括 1,存在肿瘤性坏死;2,空泡状核伴有大的核仁;3,核分裂象> 2/10HPF;4,高核浆比;5, 存在梭形肿瘤细胞;6,细胞多形性。存在 3 个或 3 个以上特征时定义为恶性颗粒细胞瘤,仅有 1 个或 2 个上述特征时归类为非典型颗粒细胞瘤,无上述任何特征者定义为良性颗粒细胞瘤。
免疫组织化学染色:
S100 弥漫强阳性, SOX10(核)、Calretinin、CD68. inhibin 及 nestin 均阳性,多数 TFE3 核阳性,细胞巢周围 IV 型胶原阳性,SMA、desmin、myogenin、GFAP、HMB-45 及 neurofilament 均阴性。
分子标记:
可见 9p 和 17p 的杂合性缺失,无 TFE3 基因重排
鉴别诊断:
颗粒性平滑肌瘤、横纹肌瘤 :肌免疫染色阳性,S100 阴性。
牙龈颗粒细胞瘤 :好发于新生儿,瘤细胞不表达 S-100 蛋白。
腺泡状软组织肉瘤: 发病年龄较清,组织学上以假腺泡状结构为主,瘤细胞可见空泡状核和明显的核仁,胞浆内可见 PAS 和 PAS-D 阳性的棒状结晶,免疫组化染色弥漫表达 TFE3,存在 TFE3 基因重排,不表达 S100 蛋白等可资鉴别。
治疗:
手术完整切除。
病例报道:
Nasser H, Ahmed Y, Szpunan SM, Kowalskia PJ. Malignant granular cell tumor: A look into the diagnostic criteria. Pathol Res Pract 2011;207:164.
参考文献:
Battistella M et al: Vascular invasion and other invasive features in granular cell tumours of the skin: a multicentre study of 119 cases. J Clin Pathol. 67(1):19-25, 2014
Chamberlain BK et al: Alveolar soft part sarcoma and granular cell tumor: an immunohistochemical comparison study. Hum Pathol. 45(5):1039-44, 2014
Gomes CC et al: Evidence for loss of heterozygosity (LOH) at chromosomes 9p and 17p in oral granular cell tumors: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol. 115(2):249-53, 2013
Izquierdo F et al: Perineurial cells in granular cell tumors and neoplasms with perineural invasion: an immunohistochemical study. Am J Dermatopathol. 34(8):800-9, 2012
Covington MF et al: Pituicytoma, spindle cell oncocytoma, and granular cell tumor: clarification and meta-analysis of the world literature since 1893. AJNR Am J Neuroradiol. 32(11):2067-72, 2011
Nasser H et al: Malignant granular cell tumor: a look into the diagnostic criteria. Pathol Res Pract. 207(3):164-8, 2011
Papalas JA et al: Recurrence risk and margin status in granular cell tumors of the breast: a clinicopathologic study of 13 patients. Arch Pathol Lab Med. 135(7):890-5, 2011
Rejas RA et al: The neural histogenetic origin of the oral granular cell tumor: an immunohistochemical evidence. Med Oral Patol Oral Cir Bucal. 16(1):e6-10, 2011
Shintaku M: Immunohistochemical localization of autophagosomal membrane-associated protein LC3 in granular cell tumor and schwannoma. Virchows Arch. 459(3):315-9, 2011
Papalas JA et al: Isolated and synchronous vulvar granular cell tumors: a clinicopathologic study of 17 cases in 13 patients. Int J Gynecol Pathol. 29(2):173-80, 2010